
Changing diabetes medication directly alters your supply requirements because different medications use different delivery systems, and insurance coverage rules follow the delivery method, not just the drug. This is the core reason why switching from one therapy to another, whether from a basal insulin pen to an insulin pump or from injectable GLP-1 receptor agonists to oral agents, triggers a cascade of supply, prescription, and billing changes. Understanding why changing diabetes medication affects supplies helps you avoid treatment gaps, unexpected out-of-pocket costs, and the frustration of having the wrong supplies on hand. The shift is rarely just about the drug itself.
Why changing diabetes medication affects supplies
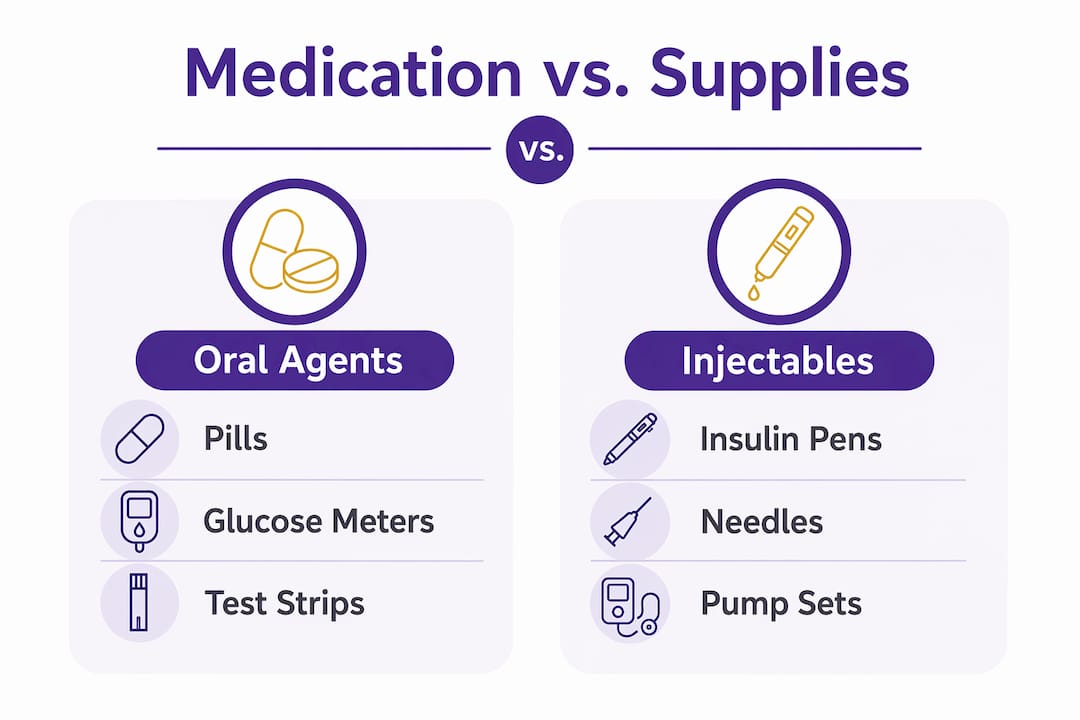
Different medications require different tools to deliver them. A patient moving from oral metformin to injectable insulin suddenly needs syringes or pen needles, a sharps container, and possibly a continuous glucose monitor (CGM) like the Dexcom G7 or Freestyle Libre. A patient switching from an insulin pen to an insulin pump needs infusion sets, reservoirs, and pump-specific cartridges. The medication change and the supply change are inseparable.
Diabetes medication intensification is driven by disease progression, side effects, or drug interactions. Adding a GLP-1 receptor agonist to metformin, for example, can reduce A1c by 1% to over 2%, which is a meaningful clinical improvement. That same switch from oral-only therapy to an injectable GLP-1 means you now need injection pens, pen needles, and potentially more frequent glucose monitoring supplies.
Here is a quick reference for common medication types and the supplies they require:
| Medication type | Delivery method | Key supplies needed |
|---|---|---|
| Oral agents (metformin, SGLT2 inhibitors) | Tablet | Test strips, lancing device, lancets |
| Basal insulin (glargine, detemir) | Pen or syringe | Pen needles or syringes, sharps container |
| Rapid-acting insulin (aspart, lispro) | Pen, syringe, or pump | Pen needles, infusion sets, reservoirs |
| GLP-1 receptor agonists (semaglutide, dulaglutide) | Injection pen | Pen needles, sharps container |
| Insulin pump therapy | Pump device | Infusion sets, reservoirs, pump batteries |
Pro Tip: When your doctor changes your medication, ask specifically which supplies the new therapy requires before you leave the appointment. Getting a supply prescription at the same visit prevents a gap in care.
The supply impact of changing diabetes drugs goes beyond convenience. Insurance plans categorize supplies based on delivery method, so a medication change can shift which plan covers your supplies and at what cost.
How insurance coverage shifts when you switch diabetes medications
Medicare is the clearest example of how delivery method determines coverage. Medicare Part B covers insulin delivered through a pump and all related pump supplies, while Part D covers insulin delivered by pen or syringe along with those supplies. Both have a $35 monthly copay cap, but they operate as completely separate benefit categories.
This distinction creates a real problem when you switch delivery methods. Moving from a pump to a pen often results in claim rejections because the billing codes and formulary categories do not automatically update. Your pharmacy may submit a claim under Part B when your new therapy is a Part D benefit, and the claim gets denied. You end up paying out of pocket until the records are corrected.
Common insurance pitfalls when transitioning diabetes prescriptions include:
- Mismatched billing codes. Pump supplies billed under Part D or pen supplies billed under Part B will be rejected.
- Formulary gaps. Your new medication or its supplies may not appear on your plan’s approved list yet.
- Missing prior authorizations. Many plans require a new prior authorization when you switch delivery methods, even for the same drug class.
- Outdated supply prescriptions. A prescription for insulin does not automatically cover the new pen needles or infusion sets you need.
- Documentation gaps from pharmacy substitutions. Pharmacists cannot legally substitute insulin brand or delivery method without a new prescription, and unsupervised substitutions create insurance claim denials down the line.
Understanding private insurance supply categories is equally important for patients on commercial plans. Private insurers follow similar logic to Medicare, categorizing supplies by delivery method and requiring updated documentation when your therapy changes.
Pro Tip: Call your insurance plan before your first fill under a new medication. Ask specifically whether the new drug and its supplies are on the formulary and whether a prior authorization is required. This one call can prevent weeks of billing delays.
How supply chain disruptions force medication and supply changes
Supply chain fragility is a major but underappreciated driver of medication switches. Manufacturer decisions, not just clinical ones, can force you to change your therapy and your supplies. Levemir insulin was permanently discontinued in 2025 with no biosimilar alternative available, requiring patients to transition to other basal insulins and obtain new prescriptions for any supplies tied to that specific product format.
Novo Nordisk also discontinued insulin aspart vials and cartridges, creating temporary shortages as biosimilars entered the market. Manufacturing scale-up for biosimilar insulins takes 2–3 years, so these disruptions are rarely resolved quickly. Patients who relied on a specific cartridge format for their pen device suddenly found themselves without compatible supplies.
The pharmacy supply chain for insulin is fragile. Manufacturer decisions can cause multi-month disruptions that affect not just the medication itself, but every supply tied to its delivery format. Patients who wait until they run out to act are the most vulnerable.
Steps to protect yourself from supply disruptions:
- Monitor manufacturer announcements. Sign up for alerts from your medication’s manufacturer or ask your pharmacist to flag any discontinuation notices.
- Maintain a 30-day buffer. Keep at least a one-month supply of your current medication and related supplies on hand.
- Ask your pharmacist about alternatives early. The pharmacist’s role in the supply chain includes identifying equivalent products before a shortage becomes critical.
- Get a backup prescription. Ask your doctor for a prescription for an alternative basal or rapid-acting insulin in case your primary medication becomes unavailable.
Managing your diabetic supplies effectively after medication changes
Proactive supply management after a medication change prevents both shortages and excess. The two most common problems are running out of the new supplies before insurance approves them, and accumulating unused supplies from the old therapy. Both are avoidable.
When you switch medications, take these steps right away:
- Notify your pharmacist immediately. Your pharmacist needs to update your medication record and flag any supply prescription changes. This prevents the documentation gaps that lead to insurance denials.
- Confirm your formulary before the first fill. Check that both the new medication and its supplies are covered under your current plan. Review how diabetes supply prescriptions work to understand what separate prescriptions you may need.
- Track your existing supply inventory. Count what you have on hand from the old therapy. Knowing your stock prevents both hoarding and shortages.
- Request updated supply prescriptions at your medication appointment. Do not assume your doctor will automatically write new prescriptions for pen needles, infusion sets, or test strips. Ask directly.
- Plan for a transition overlap period. You may need supplies for both the old and new therapy for a short time while your body adjusts and insurance updates.
Reducing supply hoarding is a real concern after medication changes. Unused supplies from your previous therapy take up space, expire, and represent money you already spent. Knowing what to do with them matters.
Deprescribing is another scenario worth planning for. A 2026 study found that safe medication reduction tied to lifestyle changes is possible, with rare adverse events when properly monitored. Patients who reduce or stop insulin after lifestyle improvements often find themselves with excess supplies that are still sealed and usable.
Key Takeaways
Changing diabetes medication triggers supply changes because delivery methods, insurance categories, and supply chain availability are all linked to the specific drug and how it is administered.
| Point | Details |
|---|---|
| Delivery method drives supply needs | Every medication type requires specific supplies; switching therapy means switching supply categories. |
| Medicare Part B vs. Part D matters | Pump insulin falls under Part B; pen and syringe insulin falls under Part D, each with separate billing rules. |
| Supply chain disruptions are real | Discontinuations like Levemir and insulin aspart formats force medication and supply transitions with little warning. |
| Update prescriptions and insurance promptly | Claim denials follow mismatched billing codes; notify your pharmacist and insurer before your first new fill. |
| Unused supplies have value | Sealed supplies from a previous therapy can be sold rather than discarded, recovering some of your cost. |
What I’ve learned from watching patients navigate medication changes
Medication changes reflect disease progression, not failure. That framing matters because patients who understand this tend to manage the supply transition far better than those who feel blindsided by it. The Cleveland Clinic is clear on this point: adjusting therapy is a normal part of diabetes management, not a sign that something went wrong.
What I find most overlooked is the insurance piece. Patients focus on the new medication and forget that their supplies now live in a different coverage category. The $35 monthly copay cap under Medicare sounds simple until you realize it applies separately under Part B and Part D, and that a billing code mismatch can freeze your access to supplies for weeks. That is a preventable problem, and it happens constantly.
The supply chain disruptions are harder to control, but not impossible to prepare for. The Levemir discontinuation caught many patients off guard because they had no buffer stock and no backup prescription. A 30-day supply buffer and a standing conversation with your pharmacist are the two most practical habits I can recommend.
Finally, do not let unused supplies from your old therapy sit in a drawer. They have real value, and there are responsible ways to recover that value rather than throwing them away.
— Liliana
What to do with unused supplies after a medication change
When a medication change leaves you with sealed, unexpired supplies from your previous therapy, you have a practical option. Orlando Diabetic Supplies Buyback buys unused diabetic supplies in Orlando, Florida, and surrounding areas, offering same-day cash for items like Dexcom G6 and G7 sensors, Freestyle Libre, Omnipod, and sealed test strips.
If you have leftover supplies from a device or therapy switch, sell your previous device supplies for fast cash instead of letting them expire unused. Orlando Diabetic Supplies Buyback makes the process straightforward: fast communication, fair pricing, and a local service you can trust. You can also learn how to get cash for any sealed supplies you no longer need. Recovering value from unused supplies is a responsible and practical step after any medication transition.
FAQ
Why does changing diabetes medication affect my supplies?
Different medications use different delivery methods, and each delivery method requires its own set of supplies. Switching from a pen to a pump, or from injectable to oral therapy, changes which supplies you need and how your insurance covers them.
Does Medicare cover supplies differently after a medication switch?
Yes. Medicare Part B covers pump-delivered insulin and pump supplies, while Part D covers pen and syringe insulin and related supplies. Switching delivery methods requires updated billing codes to avoid claim denials.
What happens to my old supplies when I switch medications?
Sealed, unexpired supplies from your previous therapy retain value. You can sell them through a local buyback service like Orlando Diabetic Supplies Buyback rather than discarding them.
Can a pharmacist substitute my insulin if it is out of stock?
No. Pharmacists cannot legally substitute insulin brand or delivery method without a new prescription. Unsupervised substitutions create documentation gaps that lead to future insurance claim denials.
How long do supply chain disruptions last after a medication discontinuation?
Manufacturing scale-up for biosimilar insulins takes 2–3 years, so disruptions following a discontinuation are often prolonged. Maintaining a 30-day supply buffer and a backup prescription reduces your exposure to these gaps.




