
You open the closet and find three boxes of test strips you haven’t touched yet. Another shipment just arrived. Sound familiar? Understanding why diabetic mail order creates surplus is not about blaming yourself or your doctor. The real causes are baked into how these programs are designed. Fixed shipment cycles, insurance quantity rules, and clinical changes that happen faster than supply systems can respond all play a role. Once you see the full picture, the pile in your closet starts to make a lot more sense.
Table of Contents
- Key takeaways
- Why diabetic mail order creates surplus through fixed cycles
- How insurance rules drive bulk deliveries and excess stock
- Clinical changes and device switches that stack up supplies
- Mail order versus local suppliers on managing surplus
- Managing your inventory and reducing the pile
- My honest take on the surplus problem
- Turn your surplus supplies into same-day cash
- FAQ
Key takeaways
| Point | Details |
|---|---|
| Mail order runs on fixed cycles | Automatic 90-day shipments continue even when your clinical needs change. |
| Insurance rules push bulk quantities | Medicare and other payers set supply limits that favor bulk delivery regardless of your current usage. |
| Device switches cause instant surplus | Changing your CGM or meter brand can make an entire supply stock incompatible overnight. |
| Surplus is a system problem | Mail-order surplus is a forecasting mismatch, not a patient error. |
| Unused supplies have real value | You can sell sealed, unexpired diabetic supplies rather than letting them expire on a shelf. |
Why diabetic mail order creates surplus through fixed cycles
Most mail order diabetes supply programs are built around one core assumption. Your needs today will be your needs three months from now. That assumption is how automatic recurring shipments work. You specify a days’ supply setting when you sign up, and the system ships on schedule, every time, without checking whether your situation has changed.
Here is what makes this a real problem in practice:
- Your 90-day shipment is packed and processed weeks before it arrives at your door.
- If your doctor adjusts your testing frequency from four times a day to twice a day, your strip consumption drops by half. But the shipment already in transit reflects the old routine.
- Insulin pump users who switch to a different reservoir size will often find their previous supplies arriving well after the switch.
- Pausing or modifying a pending order requires contacting the supplier in advance, and many patients do not realize the cutoff timeline until it is too late.
The system is built for efficiency, not flexibility. That works well when your routine is stable. It creates a growing stockpile the moment anything changes.
Pro Tip: Call your mail order supplier as soon as your doctor discusses any change in your regimen. Do not wait for the new prescription to be finalized. Early notice is the only way to stop a shipment that is already being prepared.
How insurance rules drive bulk deliveries and excess stock
This is where the surplus story gets more complicated. Insurance plans, especially Medicare, actively incentivize mail order delivery because it tends to cost less than retail pharmacy. The side effect of that cost savings is bulk quantity deliveries that do not adjust quickly to individual needs.
Medicare Part D offers three-month supplies shipped directly to your home and scheduled before you run out of your current stock. That overlap is intentional. It prevents gaps in supply. But when your therapy changes in month two of a three-month cycle, you are left with supplies you no longer need.
The quantity rules go deeper than just shipment timing. Medicare Part B sets specific coverage limits based on your insulin status.
| Patient type | Monthly strip coverage |
|---|---|
| Insulin user | Up to 100 strips per month |
| Non-insulin user | Typically 33 strips per month |
The problem arises when a patient’s insulin status changes. Someone who moves from an injectable insulin regimen to an oral medication program will suddenly have three times the strips they need per month. The insurance system cannot quickly recalibrate to that change. It takes time for new documentation, new prescriptions, and updated eligibility records to filter through. In the meantime, the shipments keep coming at the higher quantity.
Pro Tip: If your insulin status changes, contact both your doctor’s office and your mail order supplier on the same day. Ask your doctor to update the prescription quantity immediately, not just the medication type. That one step can prevent months of over-shipment.
Medicare and payers prioritize adherence and administrative efficiency. That benefits many people. For those going through clinical transitions, it creates a surplus problem that can feel impossible to stop.
Clinical changes and device switches that stack up supplies
Even when the mail order system and your insurance are working as intended, your own health journey can still create a surplus. Diabetes management changes over time. Medications get adjusted. New devices come to market. Doctors update their recommendations. Each of those changes can instantly make a portion of your current supplies obsolete.

Consider what happens when you switch from one CGM brand to another. The sensors, transmitters, and calibration strips from your old system are instantly incompatible with your new device. You might have two months of Dexcom G6 sensors in your closet the week you upgrade to the G7. Those supplies are still sealed and still valid. But you cannot use them.
The same pattern plays out in several other common scenarios:
- A change in insulin dosing, say moving from a higher daily unit count to a lower one after weight loss or a new medication, means your pen needles, syringes, or cartridges pile up faster than you use them.
- A switch from a traditional glucose meter to a CGM eliminates the need for large quantities of lancets and test strips almost overnight.
- Supply disruptions at the manufacturer level can also trigger surplus. Novo Nordisk discontinued certain insulin forms in 2025, pushing many patients to alternative formulations. Those patients were often left holding unexpired stock of the discontinued product.
The common thread in all of these situations is timing. Your clinical change happens on a specific day. The supply system moves much more slowly. The gap between those two timelines is where surplus lives.
Mail order versus local suppliers on managing surplus
Not every supply model carries the same surplus risk. Looking at the two main channels side by side shows where the differences matter most.
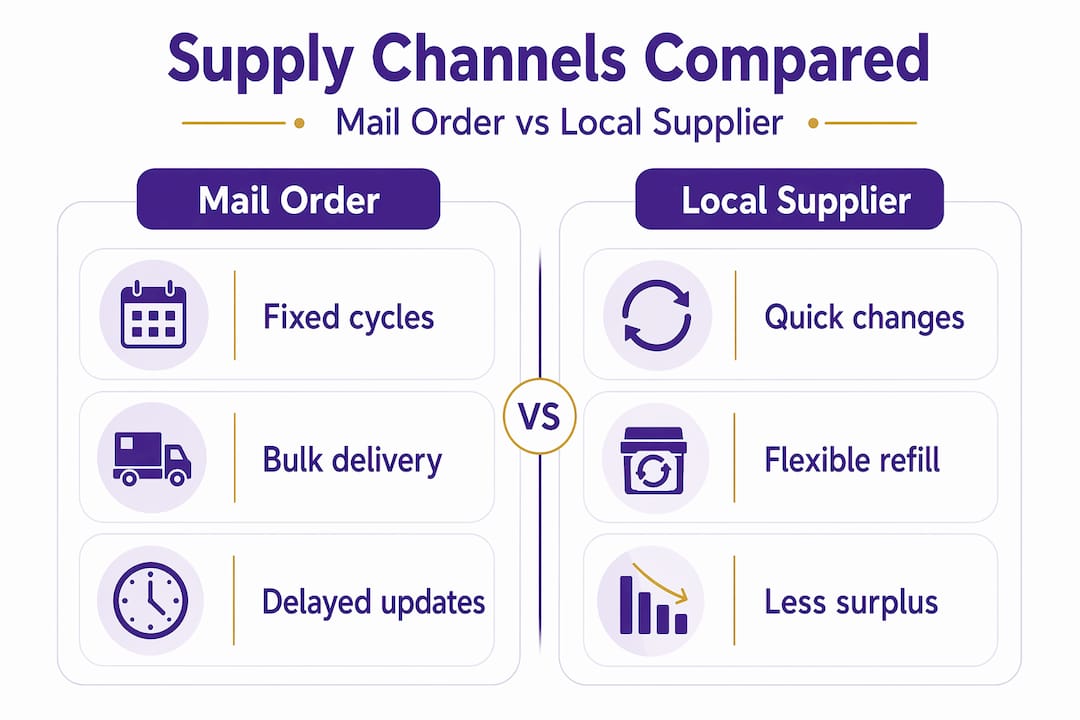
| Factor | Mail order | Local supplier |
|---|---|---|
| Shipment flexibility | Low. Fixed cycle, advance processing. | Higher. Orders placed closer to need. |
| Response to therapy changes | Slow. Requires advance notice to adjust. | Faster. Changes can often be applied same week. |
| Cost efficiency | Generally lower per unit. | Often higher per unit. |
| Surplus risk | High during clinical transitions. | Lower, due to smaller, more frequent orders. |
| Communication | Often call center based, less personal. | More direct, often with staff who know your history. |
Local providers respond quickly to prescription changes and avoid the delays that are common in mail order systems. That responsiveness reduces the surplus risk, especially during periods of clinical change.
Mail order still has real benefits. Lower cost per unit and automatic refills work well for stable patients. The trade-off is that the system is designed around stability. If your needs are predictably constant, mail order is a smart, cost-effective diabetic supplies channel. If you are in a period of change, local sourcing or a hybrid approach may serve you better.
Managing your inventory and reducing the pile
You do not have to be a passive participant in this process. There are concrete steps that can reduce how much surplus builds up and help you deal with what you already have.
- Review your days’ supply setting. Log in to your mail order portal or call your supplier and find out what quantity is set for each item. Adjusting the days’ supply parameter is the fastest single change you can make to slow down accumulation.
- Flag upcoming changes early. Tell your mail order supplier any time your doctor even mentions a possible change to your regimen. You can always cancel a hold if the change does not happen.
- Track your real usage monthly. Count how many strips, lancets, or pods you actually use in a month. Compare that to what is arriving. A two-month supply on hand is a buffer. A six-month supply is a problem building.
- Delay or skip shipments during transitions. Most mail order programs allow you to push back a scheduled shipment by two to four weeks. Use that option whenever you are between devices or medications.
- Sell sealed, unexpired surplus supplies. If you already have a stockpile, there are programs that will pay you cash for sealed and unexpired diabetic supplies. Items like Dexcom G6 sensors, Freestyle Libre sensors, Omnipod PDMs, and sealed test strips all have real value.
Pro Tip: Check the expiration dates on your current stock before your next shipment arrives. If you have supplies expiring within two months that you cannot use, contact a local buyback program first. Once they expire, that value is gone.
My honest take on the surplus problem
I’ve spent a lot of time talking with diabetics and caregivers who feel guilty about their overflowing supply closets. What I’ve learned is that guilt is the wrong response entirely.
The system is not built around your individual life. It is built around averages, administrative efficiency, and coverage rules that made sense when they were written. When your actual day-to-day reality does not match the assumptions baked into those rules, surplus happens. That is not your failure.
What I’ve found actually frustrating is how little communication flows in the right direction. The mail order company ships what the insurance says. The insurance pays what the prescription says. The prescription reflects what the doctor last documented. By the time a clinical change works its way through that chain, three more months of supplies have already arrived. The patient absorbs the mismatch. Every time.
My honest advice: treat your supply inventory like a monthly check-in, not a set-it-and-forget-it task. Look at what you have. Compare it to what you use. Act early. And if surplus has already built up, do not let sealed supplies expire on a shelf when they still have real worth.
— Liliana
Turn your surplus supplies into same-day cash
If you have sealed, unexpired diabetic supplies sitting unused, Orlando Diabetic Supplies Buyback can help you turn that inventory into real money, fast.
Whether the surplus came from a mail order cycle, an insurance over-shipment, or a device upgrade, we buy Dexcom G6 and G7 sensors, Freestyle Libre, Omnipod, and sealed test strips. The process is simple and local. You get same-day cash for supplies with no hassle and fair pricing. If you are in Orlando or the surrounding area, we are ready to help. You can also sell unused test strips if that is what you have on hand. Do not let good supplies expire. Put that value back in your pocket.
FAQ
Why does mail order keep sending supplies I don’t need?
Mail order programs run on fixed shipment cycles set when you first enrolled. Unless you proactively update your days’ supply settings or notify the supplier of a clinical change, the system ships the same quantity on the same schedule regardless of your current usage.
Does Medicare cause surplus diabetic supplies?
Yes, in many cases. Medicare Part B sets quantity limits based on insulin status, and Part D promotes three-month bulk deliveries. When your insulin status or regimen changes, those coverage rules do not update instantly, leading to over-shipment.
What should I do with unused diabetic supplies?
If your supplies are sealed and unexpired, you can sell them through a local diabetic supplies buyback program. Orlando Diabetic Supplies Buyback pays cash for unused supplies including sensors, test strips, and Omnipod devices.
Can switching CGM brands cause a big surplus?
Yes. Switching from one CGM to another, for example from Dexcom G6 to G7, makes your previous sensors and accessories immediately incompatible with your new device. Any remaining stock becomes surplus the day you switch.
How can I stop surplus diabetic supplies from building up?
Contact your mail order supplier as soon as your regimen changes, review and adjust your days’ supply settings, and consider delaying shipments during transitions. Monthly inventory checks help you catch the imbalance before it gets out of hand.